


Safe from harm
And through it all she offers me protection

Does RFK Jr have a point? I mean, not about the chemtrails or the bear carcass obviously. But there might be moves afoot on COVID vaccination which aren’t completely crazy, and I think it would be a mistake for liberals to reflexively oppose them just because of where they are coming from.
Just to be clear, none of this is a defence of the Trump administration in general. You can take it for granted that when he’s losing 9-0 on a Republican-controlled Supreme Court, the Defence Secretary is posting attack plans to the family group chat and the on-off-on-off again tariffs are adding volatility to the markets, I’m not a fan of that stuff.
And despite everyone that assured me that despite appearances the new head of the NIH (left) would be A Good Thing For Science, you can rest assured that I’m not happy to see grant funding being slashed and so on. But there are plenty of other Substacks writing on these topics already, so I don’t really see what’s gained by me adding my two pennyworth to the conversation.
On the other hand, as described by
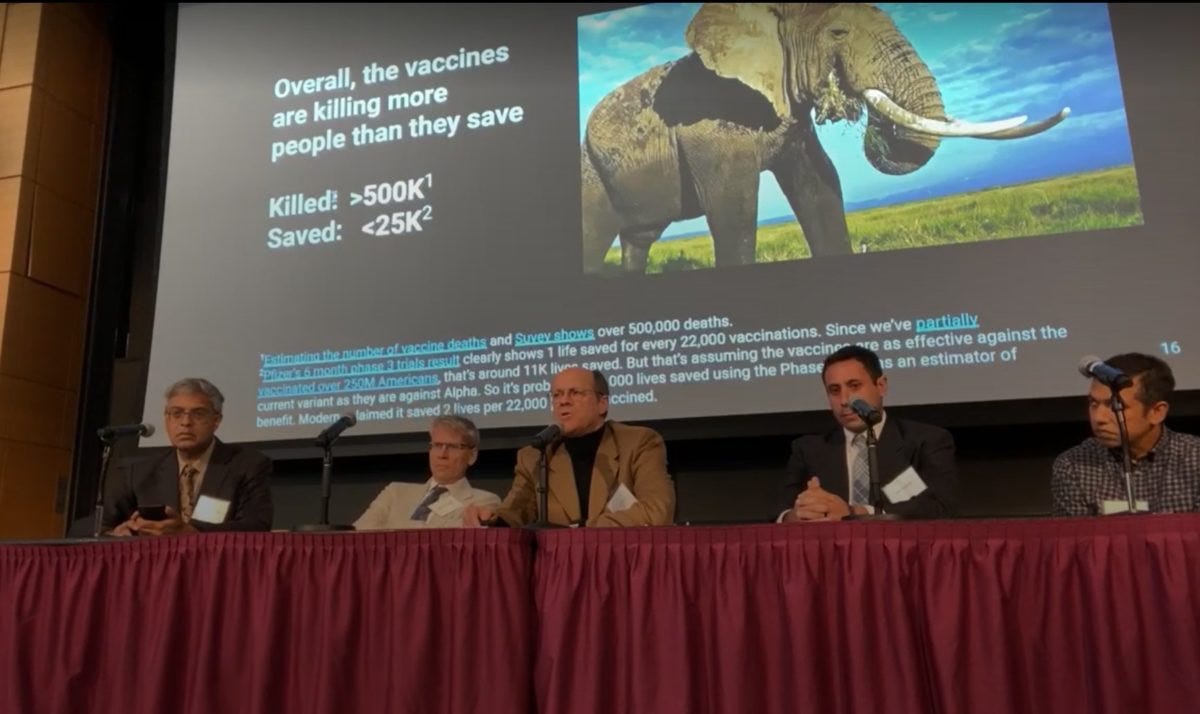
(YLE) here, the US might be moving towards a policy of risk-based vaccination for COVID, which seems entirely reasonable to me in 2025. In fact, it’s not even too hard to see why, by looking at the slide deck linked within that article.First, it’s important to say that none of what follows implies that it was a mistake to vaccinate the general population for COVID back in 2021. But as a general principle, the main reason that the novel coronavirus was so devastating was that it was novel. Our bodies didn’t have experience of dealing with it, and (see xkcd) it was generally1 better for our first contact to be via a needle than an infection. As a fiftysomething British person I got three shots back in 2021 when they were offered, and I’m glad I did because of the situation then. However, things change, and so our response shouldn’t stay set in stone forever.

And further, while this table in YLE may give the impression that countries are roughly equally split between universal and risk-based vaccination policies, it’s really the case that North America is something of an outlier in this respect. A quick google shows small variations between exact implementation, but at a quick glance broadly speaking Germany, France, Spain, Denmark and South Korea are similar to the UK in offering some version of targetting the old, those with underlying conditions, pregnant women and healthcare staff.
As I say, by looking at the slides presented in that YLE article, it’s not hard to see how these countries have arrived at this decision. We are all familiar with the idea (shown on slide 7) that there’s a steep gradient by age (and note that from slide 10 that the main proportion of risk in the big red bar for under 1s is concentrated in the “under 6 month” category - who aren’t vaccinated even under the broad-based US regime):

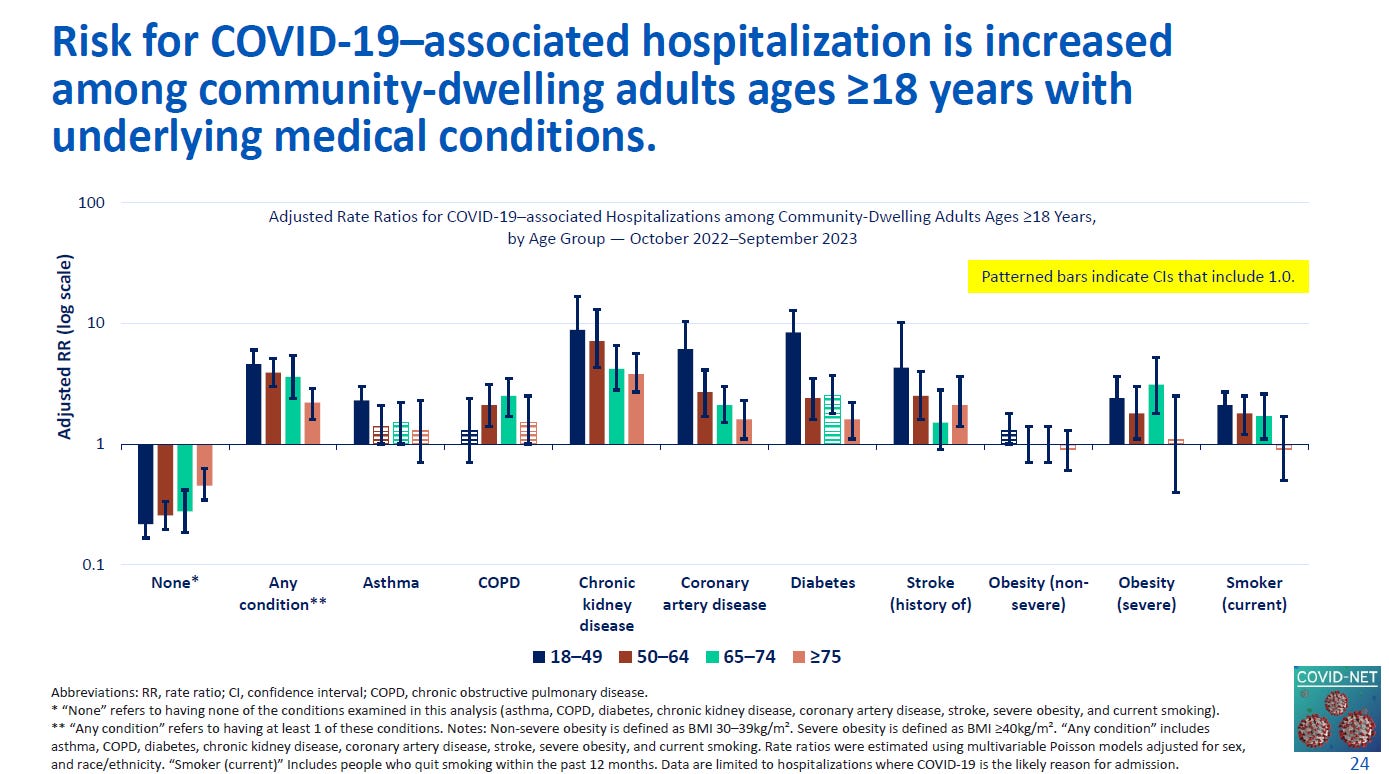
But while the hospitalization risks are already very low in younger age groups, slide 24 shows how unevenly that risk falls. Note the log scale - people with any underlying condition are about 5 times more likely than average to be hospitalized for example. So while vaccination offering a “40% added protection” against hospitalization may sound great, it’s not unreasonable to wonder what that equates to in absolute terms for people with a very low existing risk.
Taking all this into account, the UK’s Joint Committee on Vaccination and Immunisation attempted a cost-benefit analysis of the 2023-4 autumn vaccination programme. Such modelling is always somewhat uncertain, but it’s not too hard to see how they arrived at the conclusions that they did.

The estimate was that offering boosters to 50-64s as well (Option 3 instead of Option 1) would only save 10 deaths and 10 ICU admissions. Based on a population of 13 million in this age range, and an estimated £25 cost of each injection, this saving in life would come at the cost of hundreds of millions of pounds, far higher than the ten million pounds or so that standard NICE guidelines would suggest.
Indeed, while the JCVI were modelling ahead, we can check real-world data from the NHS Green Book showing a total of 159 “severe hospitalizations” in 20-49 year olds from September 2023 to September 2024 - many of which would presumably have been in the at-risk groups who were already offered a vaccine anyway.
Of course, these sums may be wrong. Other people may do the analysis another way. But I think that 5 years on, it’s not unreasonable to think that the presumption is not to keep offering boosters to these “not at risk” groups, unless someone can make a compelling case in the opposite direction.
At this stage, people are likely to point out that I’ve only focused on some of the benefits of COVID vaccination. There are benefits to preventing illness in terms of lost days at work, and I’d be happy to see a model of the amount that a universal programme could save in that sense too (bearing in mind real-world effectiveness, and the high levels of antibodies even in non-boosted groups in Figure 6 here).
And similarly, while YLE mentions that “Long Covid still exists”, I’d want to see a calculation based on both realistic current incidence rates and severity, and the likely incremental effect of further boosters to understand what the benefit of continuing universal coverage might be. Given that some of the more hyperbolic models from online COVID influencers had 60% of the population with Long COVID by now (not exactly a figure backed up by real-world observation), at the very least it’s clear that we need to put accurate data into any models though.

I’m open-minded as to what such an analysis might conclude. But I certainly think we shouldn’t assume that should just keep doing the things we did in 2021 and 2022 by default.
And there’s a bigger danger. While YLE says that “Implementing and communicating universal vaccination recommendations is much easier”, the question of COVID vaccination doesn’t exist in a vacuum. If it is really the case that these vaccines are being offered to some people with little potential benefit, that doesn’t help with messaging overall. As the US measles outbreak continues to grow, it makes it much harder to argue “you really need to give your kids the MMR” if it’s presented as part of a menu where some items are so much more important than others.
As a British person, I am perfectly happy with the JCVI’s advice - they played a blinder on delaying the second COVID dose for example - so if they think that I don’t need another booster right now, then I’m happy to assume they know more about it than I do. While I could go and pay for another vaccine, personally I don’t feel the need, even if that might put me on the same side as RFK and the rest of them for once.
Yes, I know that some people were harmed by the vaccine. Yes, I know that not all reinfections were less severe than first infections. This is a population-level statement.
Totally agree, the JCVI still seems mercifully free from ideological agendas when making its recommendations, and let’s hope it stays that way!
I hate being ill - and on those grounds alone I’ll continue getting vaccinated, paying if necessary, because it somewhat reduces my chance of getting Covid, and probably I’ll be less unwell if I do get it, and so for me it’s definitely worth it.